
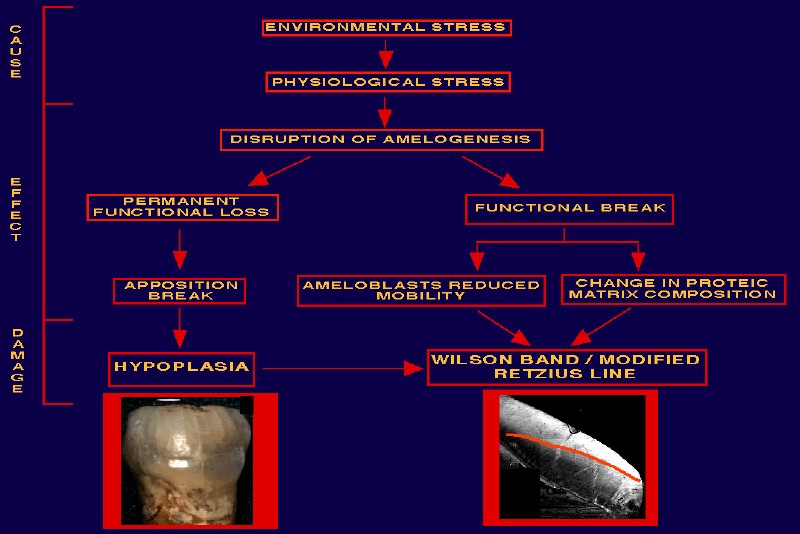
A metabolic disturbance sufficient to alter the regular growth pattern of an individual produces a corresponding disruption in the physiological function of all cells and will be recorded in the tissues as a developmental defect. Unlike bone, dental enamel does not remodel once it is formed, and it can retain a complete record of disturbances from very early on in development (i.e., the 3rd to 4th month of intrauterine life) in the form of characteristic stress markers (Levine et al., 1979; Goodman and Rose, 1990; Skinner and Goodman, 1992).
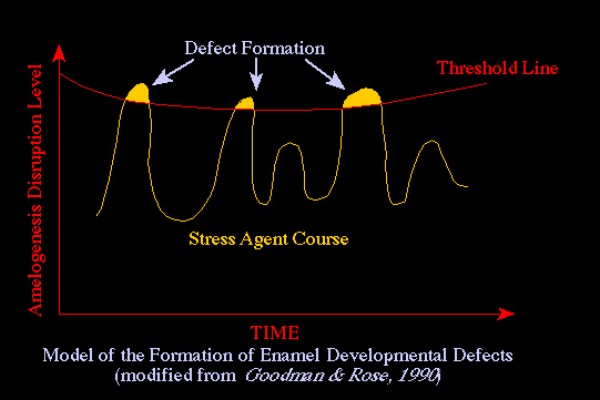
Enamel, therefore, represents a biological database potentially capable of permanently recording all the stress events that are of sufficient magnitude to reach and surpass the threshold of individual susceptibility. The high degree of sensitivity to physiological perturbations in this tissue can be explained by the extreme specialisation of its structural units (the ameloblasts).
Developmental defects of enamel can be macroscopically detected on the lingual/labial surface of teeth in the form of hypoplasias or hypocalcifications or, in thin sections across the crown, as pathological incremental lines, all of which reflect a disruption of the normal pattern of enamel formation (Massler et al., 1941; Skinner and Goodman, 1992). For both types of stress indicators, the age at which the metabolic insult occurred in a given individual can be tentatively estimated (Levine et al., 1979).
Enamel hypoplasias (quantitative defects) refer to a deficiency in the amount or thickness of enamel. These defects may range in appearance from single or multiple pits or small furrows, to deep and wide troughs (lines, bands) of decreased enamel thickness, and ultimately, to the complete absence of enamel (Goodman and Rose, 1990). These changes are usually attributed to an initial deficit in matrix formation during the secretory phase of amelogenesis.
The age of formation of the defect can be estimated by measuring the defect position relative to the cemento-enamel junction (Goodman and Rose, 1991).
Enamel hypocalcifications (qualitative defects) occur when normal mineralization is disrupted, and are manifested as bands or irregular areas of chalky, opaque, porous enamel that, over time, acquire a yellow, brown, or grey discoloration (Duray, 1990; Skinner and Goodman, 1992).
A peculiar type of surface defect of the enamel, the etiology of which is still debated, is a localised hypoplasia of the labial surface of deciduous canine (Skinner, 1986; Skinner and Hung, 1986; 1989; Lukacs, 1991; Lukacs and Walimbe, 1997).
A comprehensive classification of enamel surface defects, considering type, location, number and demarcation has been developed by Ainamo and Cutress (1982).
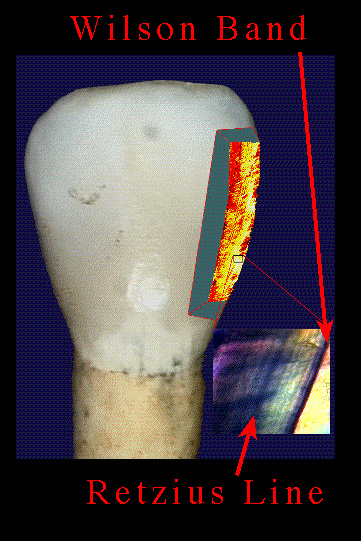
In longitudinal thin sections, stress markers occur as abnormal striae situated parallel to physiological incremental lines (Retzius lines). Abnormal striae (i.e., modified Retzius lines) are defined as pathological because of the altered morphological structure; their width is broader than that of normal physiological lines and prism structure is atypical (or even absent). Enamel microdefects follow the same path of Retzius lines from the dentino-enamel junction towards the surface of the tooth, and are named Wilson bands (Wilson and Shroff, 1970; Rose, 1973, 1977, 1979; Rose et al., 1985).
Using optical microscopy, Gustafson (1959) and Wilson and Shroff (1970) demonstrated that the striae of Retzius are related to the bending of the rods during normal development, rather than to a physiological disturbance or pause during one of the phases of amelogenesis. On the other hand, pathological bands relate to the stage when normal development of the enamel has been affected by some stimulus that has caused a sudden change in the metabolism of ameloblasts. This is indicated by the abnormal prism structure of pathological bands. The fact that the course of these broad bands is parallel to the striae of Retzius can be explained by taking into account the direction of the mineralising front of enamel.
Wilson bands are not homogeneously distributed throughout the enamel thickness, but are more frequently found in enamel that has formed postnatally. In fact, the fraction of enamel formed in utero is usually more regular in appearance as its growth is regulated by maternal physiology.
Because the pattern of enamel growth and its mean rate of deposition are known (Massler et al., 1941; Levine et al., 1979; but see also Schroeder, 1991), the age of formation of each microscopic defect can be assessed (see Sciulli, 1992) .
The degree of correspondence between macro- and microdefects, that is, between hypoplasias and Wilson bands, has been also evaluated. Massler and co-workers (1941) suggested that a disruption during amelogenesis produces a reaction in the enamel which is proportional to the severity of the injury. Accordingly, hypoplasias would indicate a severe systemic disturbance, while modified Retzius lines could also result from a mild stress.
In a comparative histological study of paired mandibular C and P3, Condon (1981a, cited by Rose et al., 1985; see also Condon, 1981b) proposed that Wilson bands should be the result of very short periods of metabolic disturbance (1-5 days), while hypoplasias should represent the involvement of a larger number of ameloblasts over a longer period of time (lasting from several weeks to two months). This hypothesis is apparently supported by the evidence that, while hypoplasias seem invariably associated with one or more Wilson bands, Wilson bands are not necessarily associated with hypoplasias.
From this perspective, pathological bands are thus considered to be more sensitive indicators of stress than hypoplasias (Skinner and Goodman, 1992).
In contrast with these findings, however, Wright (1990) and Kahru (1991) recorded a number of hypoplasias without underlying Wilson bands, a very unusual result not confirmed by our extensive study. Wright (1990) explained this pattern by suggesting that only severe episodes of stress may initiate Wilson band formation, but that they will not influence surface morphology (i.e., produce a hypoplastic defect) unless the stress continues for an extended period of time. Conversely, a prolonged mild stress may produce shallow hypoplasias without reaching a threshold level necessary for Wilson band formation. Goodman and Rose (1990) suggested that finding one possible hypoplastic line and a series of slight depressions on a tooth surface, with no associated evidence of underlying microdefects, is not representative of hypoplasia but rather of prominent perikymata. Further, Simpson (1997) showed that when the location of Wilson bands and surface defects correspond, the pathological bands are most likely to be found at the cuspal edge of the hypoplasia (i.e., corresponding with the period of onset).
Clinical research investigated the relationships between developmental (mineralization) defects of the enamel and conditions such as: neonatal asphyxia (Grahnén et al., 1969; Magnusson et al., 1978); hypocalcemia (Levine and Keen, 1974); nephrotic syndrome (Shusterman and Fellers, 1969); intra-uterine undernutrition (Grahnén et al., 1972; Norén et al., 1978b); birth weight (Norén, 1983; Norén et al., 1984; Seow, 1992); congenital hypothyroidism (Norén et al., 1984); minimal brain disfunction, mental retardation, and related neurologic disorders (Norén and Gillberg, 1987; Bhat and Nelson, 1989); maternal diabetes (Norén et al., 1978a; Norén, 1984); sudden infant death syndrome (Teivens et al., 1996). For a comprehensive overview, see Bhat and Nelson (1989).
At any rate, current available evidence shows that Wilson bands result from developmental disruptions and are easier to detect without a corresponding hypoplastic defect; this strongly suggests that enamel microdefects reflect a broader spectrum of metabolic disturbances.
Some advantages in recording micro- vs. macrodefects are evident in (paleo)epidemiological investigation: a) hypoplasias are more frequently seen in the cervical region of teeth rather than on the whole crown surface, thus limiting the information to a narrow chronological period in comparison to microdefects; b) there is a risk that surface defects will be deleted due to dental wear and/or corrosive action of saliva during the mastication process (Cook, 1981); c) in archaeological specimens, detailed features of the surface defects can be attenuated (or even removed) by diagenesis and other postmortem alterations. Conversely, microscopic developmental defects of enamel are well preserved and recognisable on thin sections, even when the external surface of the tooth is substantially damaged (Rossi et al., 1996, 1997).

